What Does a Bartholin Cyst Look Like Pictures – Symptoms, Stages & Treatment Guide
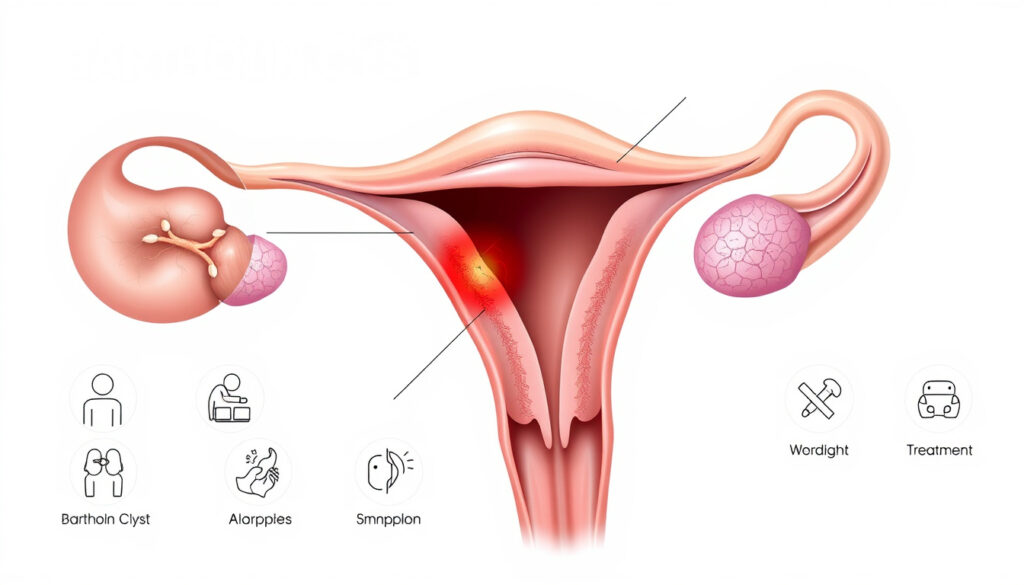
A Bartholin cyst appears as a fluid-filled lump near the vaginal opening, developing when one of the Bartholin glands becomes blocked. These glands, located on each side of the vulva, normally produce moisture to lubricate the vaginal area. When the ducts become obstructed, fluid accumulates beneath the skin, forming a growth that can range from barely noticeable to several centimeters in diameter. Understanding what this condition looks like can help individuals recognize symptoms early and seek appropriate medical guidance.
Bartholin cysts are relatively common among women of reproductive age, though they can occur at any adult age. The appearance varies significantly depending on whether the cyst remains uninfected or develops into a more serious abscess. While small, uncomplicated cysts often appear as soft, skin-colored bumps that may cause minimal discomfort, infected versions present with noticeably different characteristics including discoloration, swelling, and pain. Medical professionals stress that visual identification alone is insufficient for diagnosis, making it important to understand the typical presentation while knowing when professional evaluation becomes necessary.
This guide provides a comprehensive visual overview of Bartholin cysts across different stages and conditions, drawing from established medical sources to clarify what individuals might observe. The information presented here should support awareness rather than replace consultation with a qualified healthcare provider, particularly when symptoms cause concern or interfere with daily activities.
What Does a Bartholin Cyst Look Like?
The most characteristic appearance of a Bartholin cyst is a rounded lump situated near the vaginal opening, typically on one of the two sides. In its uncomplicated form, the growth presents as a smooth, skin-colored elevation that feels firm yet moveable beneath the surface. Most cysts measure between one and four centimeters in diameter, roughly corresponding to the size of a pea at the smaller end and a marble or golf ball at the larger extreme. The skin covering the cyst typically appears normal in color and texture, distinguishing it from infected lesions that show visible inflammation.
Early-stage Bartholin cysts frequently go unnoticed because they often develop gradually and without significant symptoms. A small cyst may be discovered accidentally during routine hygiene or a medical examination. The growth tends to remain discrete and localized, appearing as a distinct bump separate from surrounding tissue. When viewing medical photographs and diagrams, the classic presentation shows a well-defined oval or round structure positioned at the posterolateral aspect of the vaginal entrance, corresponding precisely to where the Bartholin glands sit internally.
Healthcare providers note several key visual markers that help identify Bartholin cysts from other genital bumps or lesions. The symmetrical positioning along the vaginal opening serves as one of the most reliable indicators, as cysts rarely appear in other genital regions. Additionally, the bilateral nature of the Bartholin glands means that cysts can develop on either side, though simultaneous occurrence on both sides remains uncommon. Medical imaging and examination techniques allow clinicians to confirm the diagnosis when visual assessment alone proves inconclusive.
Visual Characteristics Across Different Stages
Healthcare professionals categorize Bartholin cyst appearance into distinct stages, each with recognizable features. In the initial formation stage, the cyst presents as a tiny, often imperceptible lump that may measure only a few millimeters. The skin above remains normal in appearance, and the individual typically experiences little to no discomfort. This early phase can persist for extended periods without noticeable progression, which explains why many people never realize they have a cyst until it either grows larger or becomes infected.
As fluid continues to accumulate, the cyst enlarges and becomes more apparent upon inspection. The growth maintains its smooth, rounded contour but occupies more space beneath the skin surface. At this intermediate stage, the bump becomes visible without palpation, though the overlying skin still shows no signs of inflammation or discoloration. Movement during activities such as walking or sitting may begin to cause mild irritation, particularly with cysts exceeding two centimeters in diameter.
Common Misconceptions About Appearance
Several conditions can be confused with Bartholin cysts based on appearance alone, which is why professional evaluation matters. Vaginal inclusion cysts, for example, appear similar but form from different tissue types and occur in different locations. Epidermal cysts can develop in the genital region and mimic Bartholin growths but arise from skin structures rather than Bartholin gland obstruction. Healthcare providers emphasize that accurate diagnosis requires understanding the anatomical origin, not just the visible presentation.
Bartholin cysts specifically develop in the location of the Bartholin glands near the vaginal opening. Lumps appearing elsewhere on the vulva or vaginal canal likely represent different conditions requiring alternative evaluation approaches.
Medical Documentation Standards
Clinical photographs of Bartholin cysts serve important educational purposes in medical training and patient resources. Standard medical texts and hospital resources often include diagrams and illustrative images showing representative examples of cyst appearance at various stages. These materials typically demonstrate the relationship between the cyst and surrounding anatomical structures, helping both healthcare students and patients understand the condition’s presentation. The visual documentation follows established medical photography standards to ensure consistency and educational value.
While numerous images circulate online and in patient forums, the quality and accuracy of medical representation vary considerably. Reputable medical institutions such as the Mayo Clinic and the National Health Service provide vetted visual resources that accurately depict typical presentations. These sources tend to rely on diagrams and anatomical illustrations rather than clinical photographs, reflecting appropriate boundaries around patient privacy while still providing useful visual reference.
What Does an Infected Bartholin Cyst Look Like?
When a Bartholin cyst becomes infected, the visual presentation changes markedly from the relatively benign appearance of an uncomplicated cyst. The transition from cyst to abscess involves bacterial invasion of the blocked gland, triggering an inflammatory response that produces the characteristic symptoms associated with infection. This stage, known as a Bartholin abscess, develops in approximately one to three percent of cases annually and represents a significant escalation from the original cyst formation.
The most striking visual change during infection involves coloration of the affected area. The skin overlying the cyst transitions from its normal flesh tone to shades of red, dark pink, or even purple, depending on the severity of inflammation and the individual’s skin tone. This discoloration typically extends beyond the immediate boundaries of the cyst itself, creating a zone of inflammation that can measure several centimeters in diameter. The intensity of color often correlates with the extent of infection, with deeper reds and purples suggesting more significant involvement.
Signs of Abscess Formation
Beyond color changes, infected Bartholin cysts develop several characteristic features that distinguish them from uncomplicated growths. The skin surface becomes taut and shiny as underlying fluid accumulation increases pressure against the dermal layers. Palpation reveals a fluctuant quality, meaning the structure feels liquid-filled rather than solid. This characteristic helps healthcare providers confirm the presence of pus accumulation and guides treatment decisions regarding drainage procedures.
Visible pus formation represents another hallmark of infected Bartholin cysts. Depending on the stage of infection, pus may appear as white, yellow, or greenish material visible through the thinned skin surface. In some cases, the abscess develops a visible point where pus appears ready to drain spontaneously. Red streaking may extend from the affected area, indicating lymphatic involvement. The presence of these features typically prompts consideration of surgical intervention alongside antibiotic therapy.
Distinguishing From Other Conditions
Healthcare providers frequently need to differentiate infected Bartholin cysts from other conditions that produce similar-appearing lesions in the genital region. Skin infections such as boils (furuncles) can mimic abscessed Bartholin cysts but typically arise from hair follicle infections rather than glandular obstruction. Boils tend to be smaller, more localized, and often feature a raised pustule at their center that Bartholin abscesses lack given their deeper origin.
Hemorrhoids represent another condition requiring differentiation, though they present quite differently upon careful examination. Hemorrhoids develop from swollen blood vessels in the rectal area and are associated with bowel movements, itching, and sometimes bleeding. They do not appear near the vaginal opening and involve different anatomical structures entirely. The location specificity of Bartholin cysts, combined with their association with Bartholin gland anatomy, helps exclude hemorrhoid misdiagnosis in most cases.
An infected Bartholin cyst typically shows discoloration extending beyond its borders, whereas a localized skin boil remains more contained. The fluctuant feel and rapid enlargement over hours or days also distinguish Bartholin abscesses from other genital bumps that develop more gradually.
Changes Over Time
Abscess development follows a predictable progression when left untreated, though the timeline varies between individuals. Within hours to days of initial infection, the cyst begins enlarging rapidly, sometimes doubling in size within twenty-four hours. This rapid growth distinguishes abscess formation from the gradual expansion typical of uncomplicated cysts. The affected area becomes increasingly tender, with pain intensifying during activities that create pressure on the vulva, such as walking, sitting, or sexual intercourse.
Systemic symptoms may accompany the visible changes if infection becomes severe. Fever, general malaise, and fatigue suggest that bacteria have entered the bloodstream or that the body is mounting a significant immune response. Visible red streaking extending toward the groin or thigh indicates lymphatic involvement requiring prompt medical attention. These progression signs underscore the importance of seeking evaluation before minor cysts develop into serious infections requiring hospitalization or emergency intervention.
How Big Is a Bartholin Cyst and Where Is It Located?
Understanding the typical dimensions and anatomical position of Bartholin cysts helps contextualize their visual appearance and associated symptoms. The Bartholin glands themselves are relatively small, each measuring approximately 0.5 centimeters in diameter in their normal state. When obstruction occurs and fluid begins accumulating, the resulting cyst can expand considerably beyond the original gland size, reaching measurements that sometimes surprise individuals discovering them for the first time.
Most Bartholin cysts fall within a size range extending from approximately one centimeter at the smaller end to four centimeters in more significant cases. This translates roughly to the dimensions of a pea on the small end and a golf ball on the large end. Medical literature documents cases of what clinicians term “giant Bartholin cysts” that exceed these typical measurements, sometimes reaching six centimeters or larger. These exceptional cases typically require imaging studies such as MRI to fully characterize their extent and plan appropriate intervention.
Anatomical Position Explained
The Bartholin glands occupy a specific anatomical position that determines where cysts and abscesses appear on examination. Each gland sits deep within the tissues of the posterolateral vulva, positioned at approximately the four and eight o’clock positions relative to the vaginal opening. This means that cysts typically develop toward the back of the vaginal entrance rather than toward the front, and on the left or right side rather than centrally. The depth of the glands within soft tissue explains why cysts can grow substantially before becoming externally apparent.
The proximity of Bartholin glands to the vaginal opening explains why cysts in this location can interfere with sexual function and daily activities. During intercourse, pressure on the vulvar tissues can compress an existing cyst, causing discomfort that individuals often describe as pressure or pain deep within the vaginal area rather than surface-level irritation. Walking, cycling, and other activities that involve sustained sitting or friction against the vulva can similarly exacerbate symptoms from enlarged cysts.
Size Comparison Guide
Visual references help individuals understand the expected size range of Bartholin cysts. A common medical description characterizes smaller cysts as “pea-sized,” meaning approximately one centimeter in diameter. Medium-sized cysts might be compared to a marble or large grape, measuring around two to three centimeters. Large cysts reaching four centimeters are often described as golf ball-sized, while exceptional cases exceeding this dimension lack convenient everyday comparisons.
Size alone does not indicate severity or need for treatment. Some small cysts cause significant discomfort while larger ones remain painless. Infection status and symptom impact guide treatment decisions more than dimensional measurements alone.
Feeling Versus Appearance
The sensation produced by a Bartholin cyst often differs from what its appearance might suggest. Uncomplicated cysts typically feel smooth and round when palpated, with a soft to firm consistency that has been compared to a small water balloon beneath the skin. The overlying skin moves freely over the cyst structure, allowing healthcare providers to confirm that the growth originates beneath the dermis rather than within it. This characteristic helps differentiate Bartholin cysts from solid growths that might require more extensive evaluation.
Infected cysts feel notably different due to the inflammatory process occurring within and around the structure. The tissues surrounding an abscess become warm, tender, and swollen, creating an overall sensation of inflammation that extends beyond the cyst itself. The central portion may feel fluctuant or fluid-filled, while surrounding tissues feel indurated (hardened) as inflammation spreads. This change in texture accompanies the visible color changes and helps confirm the clinical impression of abscess formation.
When Should You See a Doctor for a Bartholin Cyst?
Medical evaluation becomes advisable whenever an individual discovers a new lump or swelling near the vaginal opening, regardless of whether pain or other symptoms are present. While many Bartholin cysts resolve spontaneously or require only conservative management, professional assessment ensures accurate diagnosis and appropriate treatment planning. The differential diagnosis for vulvar lumps includes numerous conditions ranging from completely benign to requiring specific intervention, making professional evaluation valuable for ruling out serious causes.
Certain visual and symptomatic changes warrant particularly prompt medical attention. Infection signs such as increasing redness, warmth, swelling, or the development of fever suggest abscess formation requiring drainage and antibiotics. Pain that interferes with daily activities, sleep, or sexual function indicates the need for symptom management. Any rapidly enlarging mass, particularly if accompanied by systemic symptoms, requires urgent evaluation to rule out complicated infection or other pathology. If you’re unsure about your due date, you can bereken je uitgerekende datum. bereken je uitgerekende datum
Red Flags Requiring Immediate Attention
Healthcare providers identify several symptoms that should prompt individuals to seek urgent or emergency care rather than waiting for a routine appointment. Fever exceeding 38.3 degrees Celsius (101 degrees Fahrenheit) combined with a genital lump suggests serious infection potentially requiring intravenous antibiotics. Extensive redness extending from the genital area toward the groin or thigh indicates spreading infection that could involve deeper tissues. Confusion, rapid heartbeat, or other signs of systemic illness accompanying a genital mass require emergency evaluation.
Significant pain that does not respond to over-the-counter medications and interferes with basic functioning such as sitting, walking, or using the bathroom warrants prompt medical attention. Inability to empty the bladder due to mass effect from an enlarged cyst or abscess represents a urological emergency requiring immediate intervention. These situations illustrate why visual assessment alone cannot guide treatment decisions—the functional impact of the condition matters as much as its appearance.
What to Expect During Evaluation
A medical evaluation for suspected Bartholin cyst typically begins with a detailed history covering symptom onset, progression, and impact on daily life. The physical examination focuses on inspecting and palpating the affected area to assess size, consistency, and tenderness. In most cases, visual inspection and physical examination provide sufficient information for diagnosis without additional testing. The Cleveland Clinic notes that healthcare providers can typically diagnose Bartholin cysts through examination alone.
Additional diagnostic testing may be ordered in specific circumstances. Laboratory testing can identify bacterial causes if infection is suspected, particularly testing for sexually transmitted infections that might have triggered gland obstruction. Imaging studies such as ultrasound or MRI help characterize unusually large cysts or those with suspicious features warranting further evaluation. Biopsy of the cyst wall may be performed if cancer cannot be excluded based on clinical appearance alone, though this remains uncommon for typical presentations.
Treatment Options Based on Findings
Treatment decisions depend on multiple factors including cyst size, symptom severity, infection status, and recurrence history. Small, asymptomatic cysts often require no active intervention beyond monitoring and hygiene measures. Warm water soaks (sitz baths) represent first-line home management for symptomatic but non-infected cysts, promoting natural drainage and symptom relief. This conservative approach allows many cysts to resolve without medical procedures.
Infected cysts and abscesses typically require drainage procedures performed by healthcare professionals. The specific technique depends on cyst characteristics and recurrence history, with options including simple incision and drainage, catheter placement for ongoing drainage, or marsupialization for recurrent cases. Antibiotic therapy accompanies drainage when significant infection is present, though antibiotics alone rarely resolve established abscesses without procedural intervention. The MedlinePlus resource provides detailed information about these treatment approaches.
Typical Progression Without Treatment
Understanding how Bartholin cysts typically evolve when left untreated helps individuals make informed decisions about seeking care. The natural history varies considerably between individuals, with some cysts remaining stable for extended periods while others progress through defined stages toward potential complications. This variability underscores why professional guidance proves valuable—even when symptoms seem manageable, knowing the typical trajectory helps prevent unexpected escalation.
- Initial formation: The Bartholin gland duct becomes obstructed, typically from unknown causes, leading to fluid accumulation in a developing cyst. This stage may produce minimal or no visible evidence.
- Cyst enlargement: Continued fluid collection causes gradual cyst growth, potentially reaching pea-sized or larger dimensions. Symptoms, if present, remain mild and primarily affect comfort during physical activities.
- Secondary infection: Bacteria enter the obstructed gland, triggering inflammatory response. Color changes, swelling, and pain develop over hours to days as the abscess forms.
- Abscess maturation: Pus accumulates within the abscess cavity, causing continued enlargement and increasing tenderness. Fever and systemic symptoms may develop if infection spreads.
- Spontaneous drainage or intervention: The abscess either ruptures externally with pus discharge, or medical intervention is sought for drainage and treatment.
- Resolution or recurrence: Following drainage, symptoms typically improve rapidly, though recurrence remains possible if the underlying gland obstruction is not addressed.
Not all cysts progress through every stage, and the timeline for progression varies considerably. Some cysts remain stable for months or years without significant change, while others develop infection within days of initial formation. The factors influencing progression trajectory include individual immune function, bacterial exposure, hygiene practices, and whether underlying risk factors for recurrence are present. This unpredictability represents one of the challenges in managing Bartholin cysts expectantly.
Understanding What Is Known and Unknown
Medical science has established clear understanding of several aspects of Bartholin cyst formation, appearance, and management while acknowledging limitations in other areas. This balanced perspective helps individuals understand which information they can rely on confidently and which requires ongoing medical research. The American College of Obstetricians and Gynecologists provides evidence-based guidance that reflects current medical consensus.
- Bartholin cysts develop from obstruction of Bartholin gland ducts
- Location near vaginal opening is consistent and anatomically defined
- Size ranges from pea-sized to golf ball-sized under normal circumstances
- Infection produces characteristic color changes and pus formation
- Diagnosis typically requires only physical examination
- Treatment effectiveness varies by intervention type
- Exact trigger for initial duct obstruction in most cases
- Why some cysts become infected while others remain uncomplicated
- Individual factors predicting recurrence versus resolution
- Optimal preventive measures to reduce initial occurrence
- Complete range of factors influencing cyst size potential
- Long-term outcomes for untreated versus treated cases
Medical Context and Broader Significance
Bartholin cysts represent one of the most common conditions affecting the Bartholin glands, which play an important role in female reproductive anatomy and sexual function. The glands contribute to vaginal lubrication during sexual arousal, with obstruction and cyst formation potentially affecting this function. Understanding the existence and normal appearance of these structures helps contextualize what happens when pathology develops, supporting body literacy and health awareness.
The condition occurs exclusively in individuals assigned female at birth who have functional Bartholin glands, meaning post-menopausal individuals and those who have undergone Bartholin gland removal face essentially no risk. Among reproductive-age women, the lifetime risk of developing at least one Bartholin cyst approaches two percent, making it a relatively common experience despite often remaining private due to the sensitive anatomical location. Healthcare providers report that many individuals feel embarrassed discussing genital symptoms, potentially delaying evaluation and prolonging discomfort unnecessarily.
Relationship to Other Gynecological Conditions
Bartholin cysts can be distinguished from other gynecological growths based on their characteristic location and presentation. Vaginal cysts, including Gartner duct cysts and inclusion cysts, develop within the vaginal canal rather than at the opening and typically require different management approaches. Skene’s gland cysts occur near the urethra rather than the vaginal opening and involve different anatomical structures. This positional specificity provides important diagnostic clues that healthcare providers use to confirm Bartholin cyst diagnosis.
The possibility of malignancy in Bartholin gland tissue exists but remains extremely rare. Bartholin gland adenocarcinoma accounts for less than one percent of vulvar malignancies, typically affecting older individuals and presenting as a persistent mass rather than a typical cyst. The rarity of malignant transformation should not prevent evaluation of any persistent vulvar mass, however, as early identification of rare cancers significantly improves treatment outcomes.
Credible Sources for Further Information
Multiple authoritative resources provide detailed information about Bartholin cysts for individuals seeking additional education or guidance. Healthcare organizations including the Healthline platform and academic medical centers maintain patient education materials that undergo professional review. These resources complement rather than replace professional medical advice, offering background information that supports conversations with healthcare providers.
Bartholin cysts are common and can be effectively managed with appropriate medical care. Prompt evaluation of any vulvar lump ensures accurate diagnosis and timely treatment when needed.
— American College of Obstetricians and Gynecologists
Patients considering treatment at specialized facilities may wish to research available options, including services offered at facilities such as the Coburg Family Medical Centre for general primary care or fertility-related services such as Monash IVF Embryo Transfer for reproductive health services. However, initial evaluation of Bartholin cysts typically begins with general gynecological or primary care providers who can perform appropriate assessment and provide referrals when specialized care is needed.
Key Takeaways
Bartholin cysts appear as fluid-filled lumps near the vaginal opening, developing from obstruction of the Bartholin glands that normally provide vaginal lubrication. The visual appearance varies from small, skin-colored bumps when uninfected to red, swollen, pus-filled abscesses when bacteria invade the blocked gland. Size typically ranges from pea-sized to golf ball-sized, though exceptional cases may exceed typical measurements. Location near the vaginal opening on either side of the vulva represents a consistent feature that helps distinguish these cysts from other genital growths.
Recognition of concerning features supports timely medical evaluation. Rapid enlargement, significant pain, fever, or spreading redness suggest infection requiring prompt attention. Many Bartholin cysts resolve with conservative measures including warm water soaks, while others require professional drainage procedures. Understanding what constitutes normal variation versus concerning presentation helps individuals make appropriate decisions about seeking care, ultimately supporting better outcomes through earlier intervention when indicated.
Frequently Asked Questions
How big can a Bartholin cyst get?
Most Bartholin cysts range from one to four centimeters in diameter, roughly comparable to a pea at the smaller end and a golf ball at the larger extreme. Rare cases called “giant Bartholin cysts” can exceed this range, sometimes reaching six centimeters or larger, though this remains uncommon.
What does a Bartholin cyst feel like to touch?
An uninfected Bartholin cyst feels smooth, round, and somewhat firm, similar to a small water balloon beneath the skin. The overlying skin typically moves freely over the cyst. An infected cyst or abscess feels fluctuant (fluid-filled), tender, and warm, with surrounding tissues often becoming hardened from inflammation.
Can a Bartholin cyst burst on its own?
Yes, an infected Bartholin cyst (abscess) can rupture spontaneously, releasing pus through a small opening. This often provides temporary pain relief but does not address underlying gland obstruction, meaning recurrence is possible. Rupture should be followed by medical evaluation to ensure proper cleaning and prevent complications.
How do I know if my Bartholin cyst is infected?
Signs of infection include increasing redness, swelling, warmth, and pain beyond mild discomfort. The skin over the cyst may change from normal flesh color to red, pink, or purple. Fever and pus formation indicate more significant infection requiring medical attention. Small cysts without these changes are likely uninfected.
Should I pop or squeeze a Bartholin cyst?
No. Attempting to rupture or express a Bartholin cyst yourself risks forcing infection deeper into tissues, causing more significant problems. Infected cysts require professional drainage under controlled conditions with appropriate precautions. Uninfected cysts typically do not require any intervention beyond monitoring.
Where exactly is the Bartholin gland located?
The Bartholin glands sit deep within the tissues on each side of the vaginal opening (vulva), specifically at approximately the four and eight o’clock positions if viewing the opening as a clock face. Cysts develop in these locations when gland ducts become obstructed.
Does a Bartholin cyst look like a pimple?
Not typically. While both are fluid-filled structures, Bartholin cysts develop in a specific anatomical location associated with the Bartholin glands and tend to be larger than typical pimples. The location near the vaginal opening rather than in hair-bearing areas also helps distinguish them. Skin infections like boils may more closely resemble some features of infected Bartholin cysts.
Is it possible to have a Bartholin cyst without knowing it?
Yes. Small Bartholin cysts often produce no noticeable symptoms and may be discovered only during routine medical examination. They can remain undetected until infection develops or the cyst grows large enough to cause discomfort during activities such as walking, sitting, or sexual intercourse.
More related posts
 Jack De Belin: Where Is He Now? Salary, Leaving Dragons
Jack De Belin: Where Is He Now? Salary, Leaving Dragons
 Dove Cameron: Facts, Biography, and LGBTQ Identity
Dove Cameron: Facts, Biography, and LGBTQ Identity
 Jim Belushi: What He’s Doing Now, Net Worth, Brother, and Farm
Jim Belushi: What He’s Doing Now, Net Worth, Brother, and Farm
 Nick Meaney: 2026 Injury, Departure & Career Update
Nick Meaney: 2026 Injury, Departure & Career Update
 Buster Keaton: Life, Disease, and Lost Fortune
Buster Keaton: Life, Disease, and Lost Fortune
 Best Collagen Supplement – Top Doctor-Recommended Picks
Best Collagen Supplement – Top Doctor-Recommended Picks
 Pat Rafter: Life After Tennis, Grand Slams & Net Worth
Pat Rafter: Life After Tennis, Grand Slams & Net Worth
 Brain Stem: Location, Function, and What Happens When Damaged
Brain Stem: Location, Function, and What Happens When Damaged
